Females are faced with a number of postural challenges. Some stem from physiological, genetic – structural demands, while some stem from psychosocial pressures and concerns.
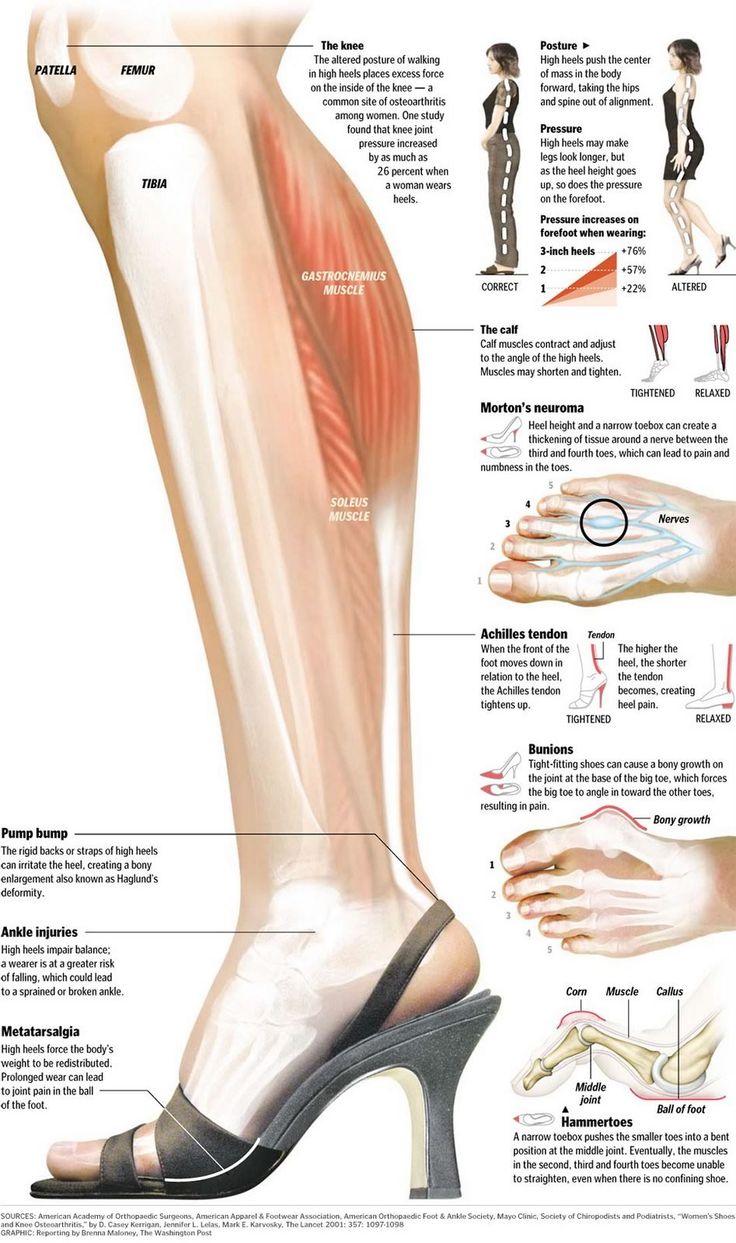
Hyperextension of the knees is a common postural fault caused by wearing high-heeled shoes.
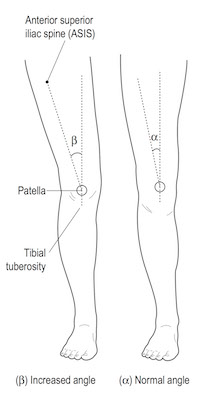
Females have a wider pelvis to support child bearing. The wider pelvis creates a larger Q angle.
 Ref: Muscle Testing and Function (4th Ed.), Kendell, McCreary & Provance.
Ref: Muscle Testing and Function (4th Ed.), Kendell, McCreary & Provance.
The Q angle is the difference between the straight line from the tibia to the hip joint, and the line of muscular action of the quadriceps represented by the angled femur (due to the attachment of the quad on the femur). Because the Q angle creates tensile stress on the MLC and compression on the lateral surface, an excessive Q angle is likely to worsen with time.
Different Q angles exist between genders: 15.8 degrees for woman, and 11.2 degrees in men. A Q-angle greater than 15 degrees is often thought to contribute to patellofemoral joint pain, chondromalacia, and patellar dislocation. The abnormal kinematic sequence between the tibia and femur may cause an increased Q-angle at the knee and an increased net lateral pull of the quadriceps or iliotibial band on the patella. These situations may predispose the patient to patellofemoral joint dysfunction. Increased Q-angle due to bony malalignment is a possible factor contributing to excessive lateral tracking of the patella. The greater the Q-angle, the greater the lateral bowstringing effect on the patella. Factors that increase the Q-angle also tend to increase genu valgum (knock-knees). Data collected at a large sports medicine clinic showed that recurrent dislocations of the patella accounted for 58.4% of all dislocations in women, compared with only 14% in men. The greater Q-angle reported in women may partially account for this large disparity.
Females have a higher incidence of joint laxity. Increased joint laxity is often associated with mechanical dysfunction of the shoulder, low back, hip, knee, ankle and foot. To determine if your client (male or female) is hyper-mobile, the Nine Point Flexibility Index Test can be performed (See under Assessment)
The degree of concern for high scores on Flexibility Index Test is directly related to the functional activities your client participates in.
Females should be encouraged to strengthen their upper bodies, with particular attention to the triceps, low back, abdominal, and elbow flexor musculature. Because of the high incidence of joint laxity in the elbow (elbow hyper extension as will be illustrated in the above test), strengthening their elbow flexors aids in stabilizing the joint.
Females are also at a higher risk of injury to the thoracic outlet, shoulder, low back, sacroiliac joints, hips, knees, ankles and feet for a number of other reasons:
1. Lack of base conditioning
2. Less muscle strength
3. Under use of closed chain exercises
4. Hormonal influence on passive joint restraints
Lack of understanding of nutrition.
Pelvic floor dysfunction is much more common in females. A number of factors could be responsible for this, these include:
1. Postural dysfunction
2. Poor abdominal conditioning technique
3. Stabilizer weakness
4. Over use of machine based exercises
5. Sacroiliac dysfunction
6. Low back pain
7. Wearing weight belts (not so commonly seen though in the female population)