
NeuroReflex is an evolution in manual rehabilitation therapy that is based on the premise that over-stimulation of the body’s primitive reflexes creates pain and dysfunction where both the reflex systems and the motor control systems are disrupted or inhibited. The NeuroReflex technique is taught on the POSTURALPERFORMANCE INSTITUTE website that covers in-depth the NeuroReflex Techniques and well as many other advanced manual therapy, rehabilitation, corrective exercise and assessment techniques.
Sir Charles Sherrington, known as the “Father of the Nervous System.” Author of the book “The Integrative Action of the Nervous System, circa 1901” established our initial understanding of the nervous system and reflexes.
Sir Charles Sherrington
Some of the principles that are applied with the NeuroReflex technique include:
1. Liddell-Sherrington reflex
2. Schiff-Sherrington reflex
3. Sherrington’s First Law
4. Sherrington’s Second Law
5. Vulpian-Heidenhain-Sherrington phenomenon
Liddell-Sherrington reflex
Associated with Edward George Tandy Liddell and Charles Scott Sherrington, the Liddell-Sherrington reflex is the tonic contraction of muscle in response to its being stretched. When a muscle lengthens beyond a certain point, the myotatic reflex causes it to tighten and attempt to shorten. This is the tension you feel during stretching exercises.
Schiff-Sherrington reflex
Associated with Moritz Schiff and Charles Scott Sherrington, describes a grave sign in animals: rigid extension of the forelimbs after damage to the spine. It may be accompanied by paradoxical respiration – the intercostal muscles are paralysed and the chest is drawn passively in and out by the diaphragm.
Sherrington’s First Law
Every posterior spinal nerve root supplies a particular area of the skin, with a certain overlap of adjacent dermatomes.
Sherrington’s Second Law:
The law of reciprocal innervation. When contraction of a muscle is stimulated, there is a simultaneous inhibition of its antagonist. It is essential for coordinated movement.
Vulpian-Heidenhain-Sherrington phenomenon
Associated with Rudolf Peter Heinrich Heidenhain, Edmé Félix Alfred Vulpian, and Charles Scott Sherrington. Describes the slow contraction of denervated skeletal muscle by stimulating autonomic cholinergic fibres innervating its blood vessels.
Primitive Reflexes
Primitive reflexes develop from conception to spur on progressive development, assist during the birthing process and enable a baby to survive the first few months of life.
Primitive reflexes are controlled by the brain stem and have a limited lifespan starting in utero and inhibiting before six months in life.
Postural reflexes are muscular reactions in opposition to the pull of gravity to maintain posture and prevent injury.
For the purposes of this article focus will be on the primitive reflexes only.
Primitive reflexes are natural reactions that:
1. Emerge to start a developmental process develop a neural circuit for a specific function integrate within the first year of life.
2. Inhibit (go to rest)
3. Re-emerge in case of injury or trauma.
Once a primitive reflex reaction has fulfilled its function – to build a specific neural pathway – it should integrate and inhibit to re-emerge should that specific pathway be injured or destroyed. Injury can occur due to exposure to radiation; foetal distress during prolonged labour; premature birth; illnesses involving high fever or convulsions; near drowning; accidents; oxygen deprivation or a stroke, to name a few.
Pain Reflex
1. Startle & Withdrawal reflexes elicited without compression over (TriggeRegions).
2. Found in many areas not associated with trigger points (see definition of trigger points below).
3. Elicits a series of groan, grab, grimace, gasp.
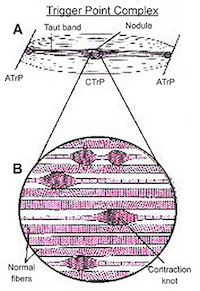
Trigger Points
1. A focus of hyper irritability in a tissue.
2. When compressed is locally tender.
3. If sufficiently hypersensitive, gives rise to:
– Referred pain
– Tenderness
– Referred autonomic phenomena
– Distortion of proprioception
Types of Trigger Points
1. Myofascial
2. Cutaneous (of, relating to, or affecting the skin)
3. Fascial
4. Ligamentous
5. Periosteal (membrane that covers the outer surface of all bones, except at the joints of long bones. Endosteum lines the inner surface of all bones.
(Reference: Travell & Simons: Myofascial Pain and Dysfunction)
The Primitive Reflexes
Withdrawal Reflex
1. Flexor reflex.
2. Nocioceptive reflex (more resent literature).
3. Not a pure flexor synergy as name suggests.
4. Polysynaptic involving multiple levels. Polysynaptic = multiple segmental of spine
5. Associated with the crossed extensor reflex in the lower extremity.
The Startle Reflex
1. Known as “Moro Reflex” in infants
2. Usually found associated with the Withdrawal Reflex in the Pain Reflex.
3. Frequently involved in Post Traumatic Stress Disorder (PTSD) as a hyper arousal response to stimuli.
4. Usually associated with an acoustic stimuli however can be visual, kinesthetic, etc.
PTSD – Trauma – Whiplash or even sport injury (if emotional component is associated)
The Micro Startle Reflex
1. Expletives said when stimulated by shock and upsets.
2. May up regulate the A.N.S. through conditioning the upset feeling to situations which we can’t or don’t control.
3. May facilitate dura through the vagus nerve.
(More woman with fibermilgra)
Difference Between Pain Reflex and Trigger Points
1. The pain reflex is elicited in an area, not a point.
2. The pattern of pain reflex has been found in hundreds of prior exams (epidodal evidence).
3. Locations are hyperalgesia which elicit the pain reflex do not correspond with trigger points.