Stability & Balance
The are two forms of stabilization that first needs to be defined and explained.
1. Segmental Stability
2. Gross Stability
Segmental Stability
Segmental stability refers to the function of stabilization of a single joint or joint complex and the ability to maintain optimal instantaneous axis of rotation (OIAR).
All of these joints are under the influence of segmental stabilizers (muscles crossing that joint only) and gross stabilizers (muscles crossing multiple joints).
The joint complex is innervated with mechanoreceptors highly sensitive to motion that provide feedback information regarding joint position, pressure, tension and pain . When the active and passive systems of the body effectively stabilize the joint complex and maintain an OIAR, normal neuromechanical relationships allow for optimal joint complex function which reflects on overall function.
Muscle imbalance, faulty recruitment of stabilizer muscles, or poor motor function decreases the ability to maintain segmental stability and an OIAR. As a result this could create an aberrant strain in the capsular and ligamentous structures of the joint complex and may cause faulty proprioceptive information to be sent to the spinal cord and brain. As a result here will be compensatory facilitation of key muscles around the involved joint complex and possibly other areas of the body.
Joint Receptors
There are 4 types of mechanoreceptors
- Type I
- Type II
- Type III
- Type IV
Type I
Low threshold, slowly adapting static and dynamic mechanoreceptors. Tonic reflexogenic effects on neck, limb, jaw and eye muscles. Postural and kinesthetic sensation. Pain suppression. Facilitate the tonic muscle system.
Type II
Fast adapting, low threshold dynamic mechanoreceptors. Phasic reflexogenic effects on the neck, limb, jaw, and eye muscles as well as pain suppression. Facilitate the phasic muscle system.
Type III
High threshold, very slow adapting receptors. Have the same characteristics as a golgi tendon organ.
Type IV
High threshold, non-adapting pain provoking nerve fibers. These fibers have tonic reflexogenic effects on the neck, limb, jaw and eye muscles. They also induce cardiovascular reflexogenic effects. Facilitation can cause guarding in the tonic muscle system.
Type I mechanoreceptors are located in the most superficial portions of a joint capsule, they are the first to be damaged any time there is of a loss of an OIAR that induces non-physiological loading of the joint capsule and ligaments. If the joint structure is damaged enough to traumatize the deeper fibers of the capsule, there will also be destruction of Type II mechanoreceptors.
Type I mechanoreceptors communicate directly with the tonic muscles of the body and the Type II mechanoreceptors communicate with the phasic muscles of the body.
Gross Stability
To maintain equilibrium during movement there is a constant activation
Stability can be defined as “resistance to both angular and linear acceleration or resistance to disruption of equilibrium”. Stabilization is the ability of the neuromuscular system to enable agonists, antagonists, synergists, stabilizers, and neutralizers to work synergistically to produce force, reduce force, and dynamically stabilize the entire kinetic chain in all three planes of motion.
Balance
Balance is defined as “the ability to control equilibrium” or “the process of maintaining the center of gravity within the body’s base of support within a given sensory environment”.
Five structural and positional factors control the degree of stability one possesses at a given time:
- Amount of body mass.
- Friction between the surface and the body in contact with it.
- Size of the base of support (BOS).
- Horizontal positioning of the center of gravity (COG).
- Vertical position of the COG.
Amount of body mass:
The more mass an object has, the more resistant it will be to a force that attempts to accelerate it. So in general objects will more mass will be more stable.
Friction between the surface and the body in contact with it:
Increased friction corresponds to increased stability as this provides better surface contact to maintain stability.
Size of the base of support:
The base of support (BOS) usually refers to the positioning of the feet. Normally, a wide stance improves stability. However, it is important to note that the size and direction of the BOS must be appropriate in light of the direction of the external force acting on an object.
Horizontal positioning of the center of gravity (COG):
For maximum stability, the COG should be on the edge of the BOS at which an external force is acting.
Vertical position of the COG:
The lower the COG, the more stable the object.
Postural Reactions
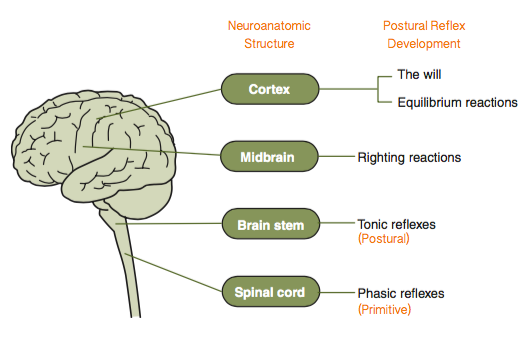
Postural reactions refers to the righting and equilibrium (tilting) response. The reflexes are the most primitive patterns that occur in response to specific stimuli, and they establish basic survival patterns of function.
- Righting Response
- Equilibrium Response (Tilting)
Righting Response
These are used primarily when we are on a fixed or stable surface. For example, if you are walking along a sidewalk and you are forcefully pushed by someone behind you, you will primarily use your righting reactions to stabilize yourself and prevent yourself from falling.
Righting reactions can be broken into five different reflexes that serve the following functions:
- Keep the head in a normal position
- Right the body to a normal position
- Adjust the body parts in relation to the head and vice versa
These reactions are called:
- Labyrinthine righting reflexes acting on the head
- Body-righting reflexes acting on the head
- Neck-righting reflexes
- Body-righting reflexes acting on the body
- Optical righting reflexes
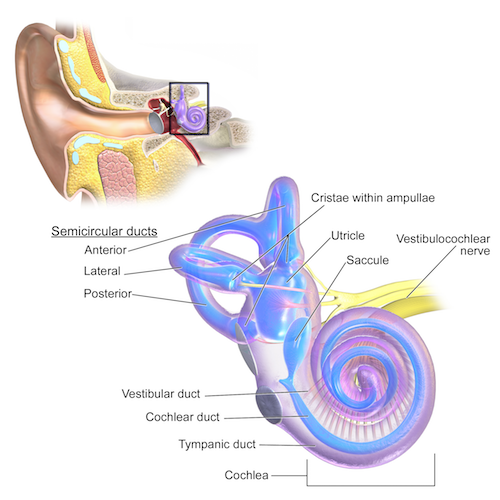
Labyrinthine-righting reflexes
The inner ear is often called the labyrinth. For this reason, the inner ear proprioceptors are often referred to as the labyrinthine proprioceptors. Stimulation of these labyrinthine proprioceptors causes changes in tone of the neck muscles via the cranial nerve (CN) VIII, which is named the vestibulocochlear nerve. As a result this brings the head into its natural position in space.
Body-righting reflexes acting on the head
Reflexive effects of the neck muscles which bring the head into the correct position in space caused by stimulation of pressoreceptors in the body wall by contact with the ground.
Asymmetrical stimulation of tactile or pressure receptors on one side of the body (such as the weight of the body lying on a table) can provide the cue for the muscular sequence which results in righting of the head in a labyrinthectomised animal. Under normal conditions this reflex must facilitate the labyrinthine righting reflexes.
Neck-righting reflexes
Changes in position of the head cause alterations in tone of the neck muscles through stimulation of proprioceptors in the labyrinth which bring the head into its correct position in space; stimulation of proprioceptors in the neck muscles in turn causes reflex movements of the limbs which bring the animal into the normal position in relation to the head.
Impulses arising asymmetrically from the neck muscles in a rotated position, result in compensatory reflexes which tend to right the body in relation to the head.
The body righting reflex
The body righting reflex is also known as the body-on-body reflex. It appears at about seven months of age and is the response of the body to pressure stimulation. The body will right itself independently of the head, so this reflex modifies the neck righting reflex. It plays a role in helping the child to move from sitting to standing.
Optical righting reflexes
This reflex is mediated in the cortex and requires intact vision and enough light in which an object can be seen. It will not function with the eyes closed or in the dark.
For our eyes to operate usefully, we need stable head control, especially when the body and head move, and also the ability to fix our gaze and follow an object. The optical righting reflex will maintain the required stability of the head, whilst the body moves, allowing the gaze to remain focused and fixed.
These require the mediation of the occipital cortex and probably need reasonable vision and visual orientation in space in the absence of other sensory cues. In normal individuals it probably has a dominant rolee, though facilitated and added to from other receptors.
Equilibrium Response
The equilibrium response is primarily primarily when the surface beneath us moves. For example, if you were taking a step off a curb and accidentally stepped onto a skateboard, in order to catch yourself from falling while the skateboard shot out from under you, you’d be primarily using your equilibrium reflexes.
These reactions are developed in us as children for the purpose of maintaining or regaining control over the body’s center of gravity, thus preventing us from falling. There are several categories of equilibrium reactions:
- Protective Reaction of the Arms and Legs
- Tilting Reactions
- Postural Fixating Reactions
Equilibrium reactions are more dominant when the supportive surface moves underneath us. Examples include wind surfing, working on a fishing boat in the open sea, riding a horse, driving a motorcycle, riding on a subway train, or riding a skateboard. These activities use righting and equilibrium reactions together, but may require a dominance of equilibrium reactions at any given moment.
Vladimir Janda stated that if we could speed the reflex response time of our bodies by 50%, we would reduce the chances of acquiring an orthopedic injury by about 80%. Due to many many environmental factors such as diet or physiological factors such as postural distortion patterns it is likely than many clients will have poor reflex responses that would could result in an increased risk of injury.