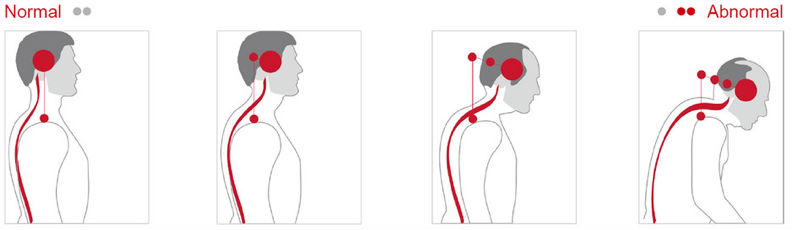
Forward Head Posture
The Forward Head Posture is characterized by characterized by increased flexion of lower cervical and the upper thoracic regions, increased extension of the occiput on the first cervical vertebra and increased extension of the upper cervical vertebrae.
There may also be Temporomandibular joint dysfunction (TMJD) with retrusion of the mandible.

Symptoms and Associated Disfunction
- Increased first rib angulation
- First-Rib Fixation Syndrome
- Thoracic outlet syndrome
- Breathing disorders
- Thyroid disfunction
- TMJ disfunction
- Fibromyalgia
- Lower-Cross Syndrome
- Dowagers Hump
- Headaches (often a symptom associated with the disorders above)
Potential Sources of Pain
Stress to the anterior longitudinal ligament in the upper cervical spine and posterior longitudinal ligament in the lower cervical and upper thoracic spine.
Muscle tension or fatigue.
Irritation of the facet joints in the upper cervical spine.
Narrowing of the intervertebral foramina in the upper cervical region, which may impinge on the blood vessels and the nerve roots, especially if there are degenerative changes.
Impingement on the neurovascular bundle from anterior scalene muscle tightness (thoracic outlet syndrome).
Impingement of the cervical plexus from levator scapulae muscle tightness.
Impingement on the greater occipital nerves from a tight or tense upper trapezius muscle, leading to tension headaches.
emporomandibular joint pain from faulty head, neck, and mandibular alignment and associated facial muscle tension.
Lower cervical disk lesions from the faulty flexed posture
Potential Muscle Impairments
Decreased flexibility in the levator scapulae, sternocleidomastoid, scalene, and suboccipital muscles. If the scapulae are elevated, there may also be tight upper trapezius muscles. With temporomandibular joint symptoms, the muscles of mastication may have increased tension.
Stretched and weakened throat muscles (hyoid becomes fixed because of the stretched position) and lower cervical and upper thoracic erector spinae muscles.
Common Causes
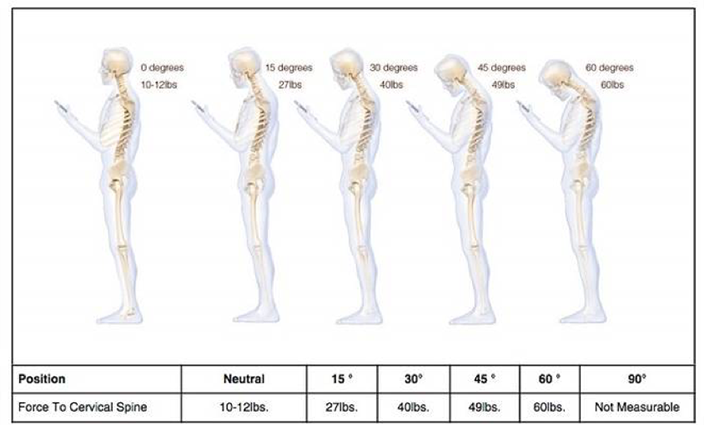
Occupational or functional postures requiring leaning forward or tipping the head backward for extended periods, faulty sitting postures such as working at an improperly placed computer screen, relaxed postures, or the end result of a faulty pelvic and lumbar spine posture are common causes of forward head posture.
A more modern phenomenon is know as “text neck” with the introduction of smart phones and tablets.
Flat-Neck Posture
The Flat Neck Posture is characterized by a decreased cervical lordosis and increased flexion of the occiput on atlas (this is an exaggeration of axial extension). It may be seen with an exaggerated military posture (flat upper back). There may be temporomandibular joint dysfunction with protraction of the mandible.
Potential Sources of Pain
Temporomandibular joint pain and occlusive changes.
Decrease in the shock-absorbing function of the lordotic curve, which may predispose the neck to injury.
Stress to the ligomentum nuchae.
Potential Muscle impairments
Decreased flexibility of the anterior neck muscles.
Theoretically, the levator scapulae, sternocleidomastoid, and scalene muscles become stretched and weakened.
Common Causes
Exaggeration of the posture for extended periods of time. This posture is not as common.
Scoliosis
A spine affected by scoliosis shows evidence of a lateral or sideways, curvature, and a rotation of the back bones (vertebrae), giving the appearance that the person is leaning to one side.
In most (80 to 85 percent) cases, the cause of scoliosis is unknown – a condition called idiopathic scoliosis. Scoliosis is more common in females than males.
Terms that describe the direction of the curve:
Dextroscoliosis describes a spinal curve to the right (“dextro” = right). Usually occurring in the thoracic spine, this is the most common type of curve. It can occur on its own (forming a “C” shape) or with another curve bending the opposite way in the lower spine (forming an “S”).
Levoscoliosis describes a spinal curve to the left (“levo” = left). While common in the lumbar spine, the rare occurrence of levoscoliosis in the thoracic spine indicates a higher probability that the scoliosis may be secondary to a spinal cord tumor. A physician will order an MRI for a thorough diagnosis.
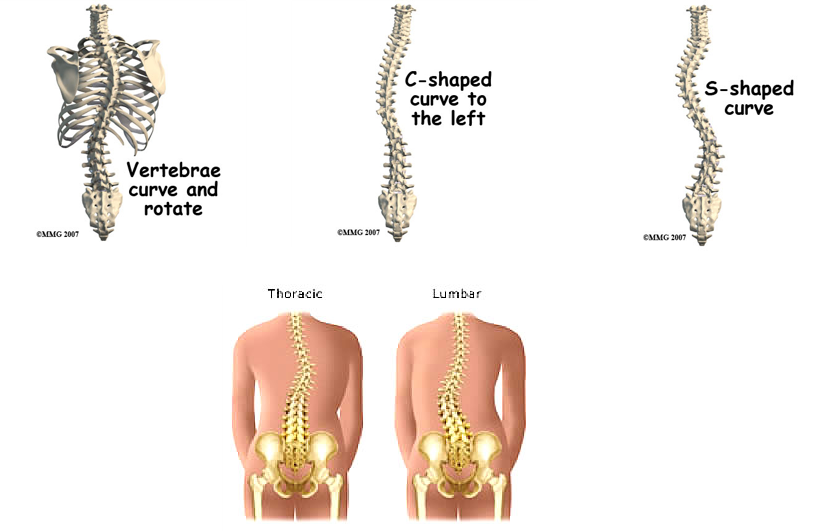
Thoracic scoliosis is curvature in the middle (thoracic) part of the spine. This is the most common location for spinal curvature.
Lumbar scoliosis is curvature in the lower (lumbar) portion of the spine.
Thoracolumbar scoliosis is curvature that includes vertebrae in both the lower thoracic portion and the upper lumbar portion of the spine.
Pes Planus (Flat Foot)
Many cases of pes planus are also marked by foot pronation, a state in which the talus protrudes medially and increases the contact area of the foot with the ground.
Flat foot impairs the body’s shock absorption mechanism and creates motor difficulties in functions or activities requiring balance and stability.
Hyperpronation may also have functional chain reaction effects throughout the lower extremities, the pelvis and the back.
Flat foot is a disorder that may result from several factors:
– Structural misconfiguration of the foot bones
– Impaired functioning of the supportive ligaments of the foot joints (because of hyperflexibility)
– Weakness of intrinsic muscles that help to maintain the foot arches
– Developmental factors
– Genetic factors
– Hypermobility of the subtalar joint.
Pes Cavus (Increased Arches)
This disorder is characterized by increased foot arch height and usually by inversion of the subtalar joint as well.
High arch is a less common disorder than flat foot.
Because of the heightened arch, foot contact with the ground is smaller than normal, thus creating an unbalanced weight distribution.
As a result, existing support points are subjected to greater pressures from loads bearing down on them
Over-inversion may also impair the foot’s ability to adjust to different surfaces while walking
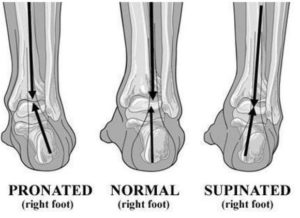
Pes Valgus (Pronated Foot)
Because the structural formation of the ankle joint facilitates movement mainly on the sagittal plane (plantar and dorsi-flexion), pes valgus with its concomitant eversion occurs in essence in the foot, in the joint between the talus bone and the calcaneus bones (subtalar joint).
This disorder is characterized by a “sinking” of the medial border of the foot to a low flat position, which exposes its lateral border to excess load.
Most cases of pronated foot are related to pes planus (flat foot).
Pes Varus (Supinated Foot)
Reverse of pes valgus or pronated foot.
The foot is in a state of inversion and most of the load is exerted on the medial border of the foot.
Hallux Valgus
Hallux Varus
Hallux varus is a deformity of the great toe joint where the hallux is deviated medially (towards the midline of the body) away from the first metatarsal bone. The hallux usually moves in the transverse plane.