
Tonic and Phasic Musculature Relationships
Understanding tonic and phasic (postural and stabilization) musculature relationships become vital when prescribing any program designed to improve flexibility or correct muscle imbalances.
This system of classifying musculature relationship for the purpose of evaluating muscular imbalances was first developed by Dr. Vladimir Janda, a Czechoslovakian physiatrist and physiotherapist. Through his research, Janda found that muscles could be divided into two functional divisions:
1. Postural (Tonic)
2. Stabilization (Phasic)
Latter research indicated that some muscles may actually fall into a third category where they may demonstrate mixed characteristics. This may occur when the muscle is expected to compensate another muscle of different classification.
Properties of Tonic and Phasic Musculature (Adapted from: Stretching and strengthening exercises, Thieme 1991)

Functional Divisions of Muscle Groups
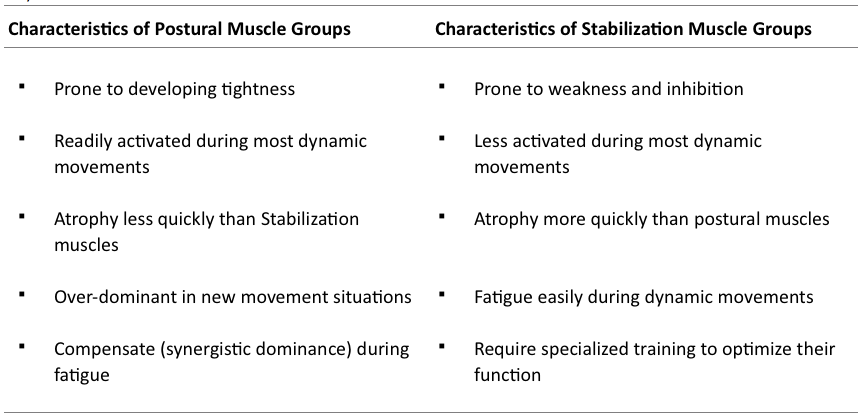
As illustrated below muscles can be generally divided into three groups according to their function as illustrated below.
Postural & Stabilization Group Musculature Relationships.

If the postural group musculature becomes shortened or facilitated it can inhibit or will try to take over the function of its stabilization group antagonists and synergists. This can prevent maximal activation of the stabilization group muscles and lead to overuse injury in the facilitated postural group muscle.
The significance of the above is that in the presence of segmental dysfunction or disturbance, the postural group muscles tend to shorten, whereas the stabilization group muscles responsible for movement tend to weaken. This situation alters the relationship between muscle and fascia, leading to imbalance and articular compensations.
(Davis Law: If muscle ends are brought closer together, then the pull of tonus is increased, thereby shortening the muscle, which may even cause hypertrophy. If muscle ends are separated beyond normal, then tonus is lessened or lost, thereby “weakening” the muscle.)
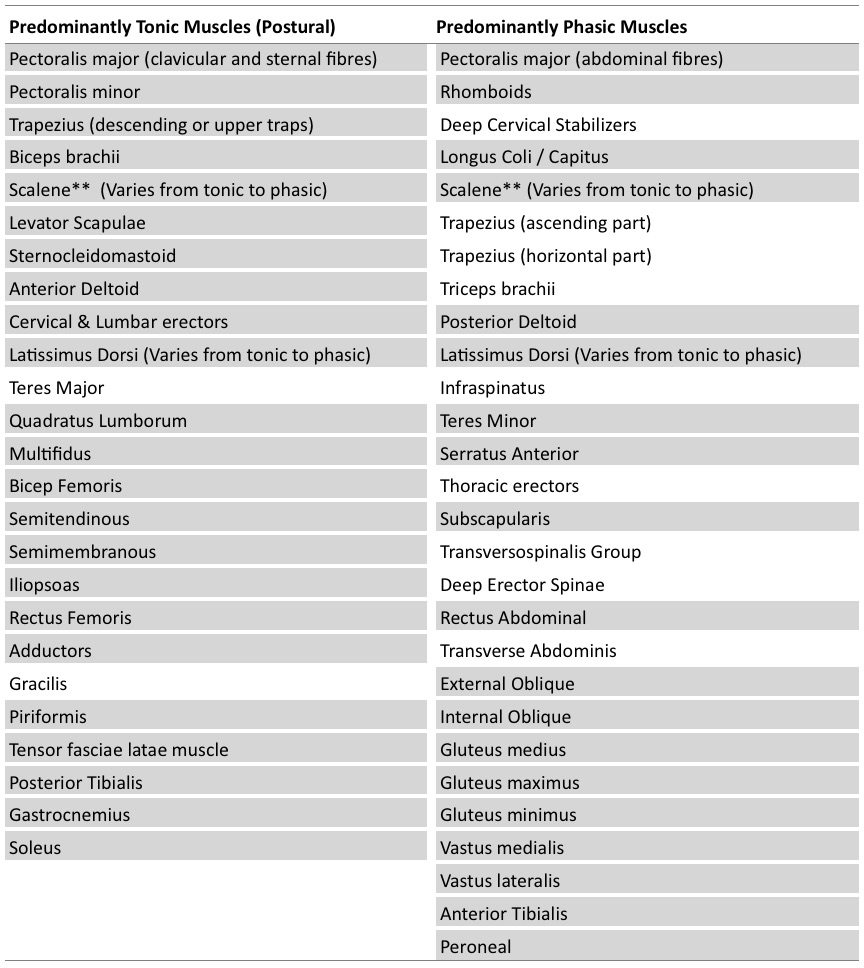
Most muscles are neutral in regards to shortening and weakening (mixed musculature). However the following table lists those muscles that have a predominantly postural (shortening) or stabilization (weakening) reaction. Those highlighted indicate the muscles identified by Dr. Janda (1983) in his research; the others were indicated in latter research.
Classification of Tonic and Phasic Muscles (Adapted from: Muscle function testing. Janda, V (1983) Butterworths;
Stretching and strengthening exercises, Thieme 1991.)
These muscles are often grouped as paired antagonists and appear to be affected by Sherrington’s Law of Reciprocal Inhibition. Thus if a tonic muscle such as psoas becomes shortened from overuse, not only will it mechanically limit the range of motion of its antagonist, the gluteus maximus, but also it will neurologically inhibit its action as well.
(Sherrington’s Law: When a muscle receives a nerve impulse to contract, its antagonists receive, simultaneously, an impulse to relax)
The condition of muscular imbalance is found when there is this lack of balance between the postural and stabilization musculature groups.
Muscle shortness or tightness, which is generally associated with postural musculature develops without any evident structural neurological lesion and is apparently associated with overuse of the particular muscle, has never been properly defined.
It indicates a condition in which the muscle is shorter than normal at rest and cannot be stretched either passively or actively to its normal length. Such a shortened muscle may move the joint from the normal rest position when inactive and does not allow full range of motion.
The important point is that a tight muscle, evidently in keeping with Sherrington’s law of reciprocal innervation, inhibits its antagonistic counterpart. This will then lead not only to muscle imbalance, but if not considered also substantially influences the effect of therapeutic or corrective exercise (Janda 1978).
The result of decreased muscle flexibility is not only a lower excitability threshold, but also a changed elasticity, evidently due to hypertrophy and retraction of the retractile connective tissue in the muscle. This hypertrophy and retraction unfavourably influences the contractile ability of the muscle fibres. In addition, it may lead to impaired circulation producing ischemia and thus accelerating degeneration. Ultimately, the whole process results in a functional disability. However, it has to be noted that histological studies of tight muscles demonstrating these phenomena are still lacking.
The vicious circle can be described as follows: during training and/or prolonged overuse, the muscle will get shorter, stronger and readily activated. However, the more marked the tightness, the worse the biomechanical and nutritional conditions of the muscle, and thus gradually the muscle strength decreases. Thus a tight muscle results in weakness, and we are right to speak about a tightness weakness. In time, adequately performed stretching may restore muscle strength.
Stretch weakness which is generally associated with stabilization group musculature was first described by Kendall (Page 334: Kendall, McCreary, Provance: Muscle Testing & Function 4th edition; Williams & Wilkins, 1993). It is defined as the effect on muscles of remaining in an elongated condition beyond the neutral physiological rest position, but not beyond the normal range of muscle elongation. According to Sahrmann (1987), a more accurate term is positional weakness.
A shortened (tight) muscle may cause an altered position of a joint which in turn may lead to elongation of its antagonist. To some extent Janda (1969, 1984, 1986) and in particular Sahrmann (1987) have developed their concepts of muscle imbalance based on Kendall’s observations. Data on experimental animals reveal that a muscle shortness is associated with shorter muscle fibres (Gossman, Sahrmann & Rose 1982), whereas an elongation of the muscle is associated with elongation of muscle fibres but decrease and shortness of sarcomeres (Tardieu et al 1979). The clinical result is, however, the same weakness.
The question is whether the final muscle weakness (due either to tightness or elongation) can be explained by this theory alone. In addition, nervous regulatory mechanisms (mainly spinal or segmental) also might participate (such as Sherrington’s law considering reciprocal innervation). In such a case, a positional weakness would be rather the result of a reflex inhibition than of impaired muscle length.
Tightness-weakness and stretch-weakness may very often appear simultaneously in functionally related muscles and play an important role in the concept of muscle imbalance however, even as regards the term muscle imbalance there is some confusion. Janda (1964) considers muscle imbalance as an impaired relationship between muscles which are prone to develop tightness and shortness (tonic) and muscles which are prone to inhibition (phasic). Under the term muscle imbalance, therefore, a combination of at least three factors should be considered:
1. Muscle length
2. The irritability threshold of specific muscles
3. Altered recruitment of those muscles
Sahrmann (1987) and, similarly, Cailliet (1977) define muscle imbalance as a failure of the agonist-antagonists relationship. Sahrmann (1987) considers muscle imbalance as active when one of a synergistic pair of muscles predominates during a movement. The result is either a diminished participation of the other muscle that leads to disuse atrophy, or excessive motion in the direction of another action produced by the dominant muscle.
Regardless of the explanation of a possible mechanism, some muscles typically develop inhibition, expressed by their hypotonia, decreased strength and (and this is particularly important) delayed activation during important movement patterns. If such a situation lasts long (several months) a mild atrophy may develop.
All these changes are not limited only to interplay between two antagonists, but have a striking tendency to generalize. In the end, a generalized muscle imbalance develops. As far as body mechanics and joint protection are concerned, muscle imbalance probably presents a much greater danger for the joint system than the muscle weakness alone.
This shortening and lengthening can be assessed by specific length and tension assessment and movement screen, these include goniometric assessment that is covered in more depth in section 4. Strength & tension assessment can be used to determine the weakened or inhibited phasic muscles however this subject is not covered in this seminar.
Muscular imbalance reduces exercise tolerance. The shortened tonic muscles engage more rapidly to produce defensive and protective movements over the phasic muscles. This can lead to short-term overloading and can increase the risk of strains or tears and the formation of myofascial trigger points in the shortened tonic musculature. Local muscular imbalance increases stress on joints and spinal segments.
The inability to move is often attributed to weakness when it may instead be a problem of chronic shortening. A muscle with a shortened resting length has neither optimal concentric or eccentric action. Because it lacks the give and take of normal muscle tissue its ability to exert force is restricted. The long back muscles (erector spinae, postural) are an excellent example. If they are tight, back extension will be limited but so will back flexion. This is an example of a limitation in movement caused by shortened, rather than weak muscles. As described above Janda (1994) describes this phenomenon as “tightness weakness.” The shortened postural muscle’s inability to deliver an adequate contraction exhibits weakness due to tightness. If you test only for strength and not length, the training protocol will be less effective.
To add even more confusion to the topic it has been found that postural muscles and phasic muscles can change from one form into the other (as indicated on the Classification of Tonic and Phasic Muscles table above) .
While Lewit and Janda (Lewit 1999) have suggested that postural muscles under stress will shorten, and phasic muscles similarly stressed will weaken, it is now becoming clear that the function of a muscle can modify its structure.
This helps to explain some mysteries – for example why the scalenes** are sometimes short, and sometimes weak, and sometimes both, and yet are classified generally as phasic muscles, and sometimes as ‘equivocal’ (maybe postural and maybe phasic).
With the research that has gone into this area, the implication is that if a group of muscles such as the scalenes are dedicated to movement (which they should be) and not to stabilisation (which they may have to be if ‘postural’ stresses are imposed), they can become postural in type, and so will develop a tendency to shorten if stressed. This is precisely what seems to happen in people with chronic upper-chest breathing patterns or asthma.
The principle of phasic and tonic musculature relationship offers a systematic approach to address muscular imbalances. As Janda suggests, before any attempt is made to strengthen weak muscles, any hypertonicity in their antagonists should be addressed by appropriate treatment which relaxes (and if appropriate lengthens) them – for example, by stretching using Neuromuscular or Static stretching techniques.