
Median Nerve Assessment – ULNT1
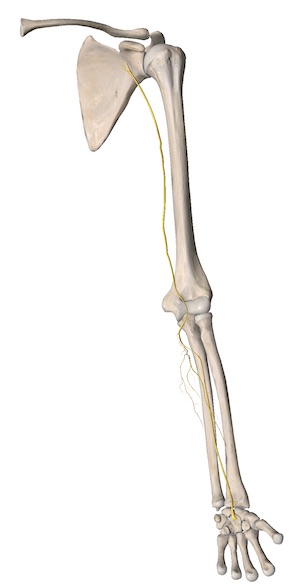
Median nerve (C5-T1)




Starting position:
- Patientlayssupine,armsbytheside,andshoulderclosetotheedge of the examination table, no pillow if possible, and body straight.
- Therapistfacesthepatient’sheadandpressesnearhandonthetable above the patient’s shoulder in either a knuckles or fist position (avoiding downward or caudad pressure on the superior aspect of the patient’s shoulder).
- Withotherhand,therapistholdspatient’shandwiththethumb extended to apply tension to the motor branch of the median nerve.Therapist’s fingers wrap around the patient’s fingers distal to the metacarpophalangeal joints.
- Patient’selbowisflexedat90degreesandsupportedonthe therapist’s near (front) thigh.
Movement sequence:
- Glenohumeralabductionupto90to110degrees,ifavailable,inthe frontal plane.
- Wristandingerextensionandforearmsupination.
- Glenohumeralexternalrotationtoavailablerange(generallystopped at 90 degrees if the patient is very mobile).
- Elbowextensionshouldbedonegentlyandwithcarenottocause any shoulder motion, especially adduction (which would ease off developing neurodynamic test).
Structural differentiation:
- Basedonwherethesymptoms(ifany)arelocated.
- Ifdistalsymptomshavedeveloped(e.g.,forearmandwristpain),the neck is moved into contralateral lateral flexion and any change in the distal symptoms would constitute a positive structural differentiation.
- Ifproximalsymptomshavedeveloped(e.g.,neckandshoulderpain), the wrist is released from its extended position and any change in the proximal symptoms would constitute a positive structural differentiation.
Palpable areas:
- Upper arm
- Medial to the biceps tendon
- Indirectly at the carpal tunnel
Common entrapments / syndromes:
- Carpal tunnel syndrome
- Post Colles’ fracture symptoms
- C5-6 nerve root